
Most Specialists Look at the Organ They Treat. Except One.
Non-member post. For educational purposes only. Published on May 14, 2026.
Every medical specialist looks at the organ they treat before deciding how to treat it. Psychiatry never has. This article examines why - and what the science says about what we're missing. For high-performers who apply rigorous thinking to their health and are ready to ask harder questions about their brain.
Sarah Parkins, founder of Birch Cove, is studying the clinical track of the Elite Brain Health program at Amen University. Through this work, she is exploring the established and evolving field of brain health in the context of business performance, examining how cognitive, emotional, and physiological wellbeing may support clearer decision-making, resilience, and sustainable leadership performance
This is not medical advice or guidance. Always consult your healthcare provider for your health needs.

The brain governs everything - cognition, mood, decisions, relationships, performance. So why is it the one organ medicine rarely looks at before treating?
Every medical specialist looks at the organ they treat before deciding how to treat it. A cardiologist images the heart. A neurologist scans the brain. An orthopedic surgeon orders an MRI before considering surgery on a knee. Across every branch of medicine, the starting point is the same: look before you treat.
There is one specialty where this has never been the standard.
In psychiatry, a diagnosis is built on what you report, how you present, and how your symptoms map onto a checklist. No scan is ordered before an antidepressant is prescribed. No image is reviewed before a diagnosis of ADHD, bipolar disorder, depression, or anxiety is given. The DSM - the Diagnostic and Statistical Manual of Mental Disorders, the manual that defines every psychiatric diagnosis by observable symptoms with no biological testing required - tells us what a condition looks like from the outside. It says nothing about what is actually happening in the brain.
In no other area of medicine would this be considered a complete clinical picture. In psychiatry, it became the standard. And it has rarely been questioned.
The Organ No One Looks At
Think about what that means in practice. The brain governs every function of human life: cognition, mood, impulse control, sleep, decision making, emotional regulation, memory, motivation. When something disrupts those functions, we call it a mental health condition and we treat it, almost always, without ever looking at the organ responsible.
SPECT imaging changes that. SPECT stands for Single Photon Emission Computed Tomography. Unlike an MRI, which shows brain structure, SPECT measures blood flow and activity. It shows the brain functioning in real time: which regions are active, which are under-active, and which are caught in patterns of over activation. It makes visible what symptom based diagnosis can only infer.
And what it shows us is that the same diagnostic label can conceal entirely different biological realities.
One Label, Seven Brains
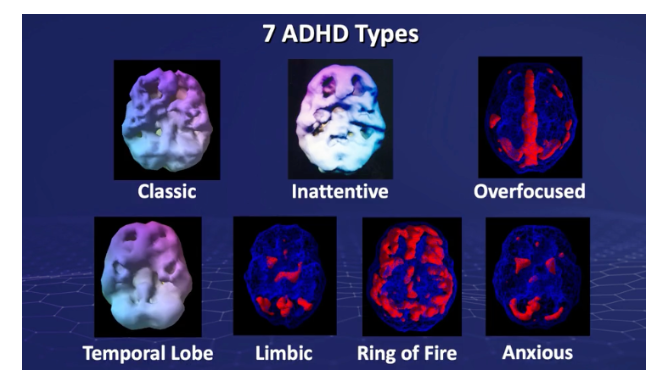
Seven neurologically distinct ADHD presentations, visible on SPECT. One diagnostic label.
ADHD is one of the clearest examples of why this matters. Imaging research has identified at least seven neurologically distinct subtypes: Classic, Inattentive, Over focused, Temporal Lobe, Limbic, Ring of Fire, and Anxious. Each has its own pattern of brain activity. Each responds differently to treatment. A stimulant medication that produces real improvement in one subtype can make another significantly worse.
Every one of those patients might walk into a clinical appointment describing broadly similar experiences: difficulty concentrating, problems with follow through, impulsivity, restlessness. Without imaging, the neurological differences between them are invisible. The distinction between Classic and Overfocused and Limbic does not exist at the level of behaviour. It only becomes visible when you look at the brain.
The same is true of depression. Two patients with identical diagnoses can show opposite patterns on a SPECT scan. One brain shows significantly reduced activity. The other shows extensive overactivation. Same reported experience, same label, opposite underlying neurology. The treatment approach that helps one may be entirely ineffective for the other. Without imaging, there is no way of knowing which you are treating.
The same logic extends to autism, anxiety, OCD, and beyond. Conditions that look the same on the surface can reflect completely different biology underneath. What appears to be one thing is often several distinct things sharing a name.
The Scale of a Problem We Have Not Solved
The outcomes data makes the gap impossible to ignore. Since 1999, the US suicide rate has increased by 35%. It is the second leading cause of death among people aged 10 to 34 in this country. In the same period, cancer mortality has declined by 27%. Cancer research made a fundamental shift toward understanding the biology of the disease: imaging, biomarkers, targeted therapies built on detailed knowledge of what was actually happening in the tissue. Mental health, by and large, did not make that shift. The diagnostic framework stayed descriptive. The treatments stayed largely the same.
The prescribing picture reflects this. In 2022, approximately one in five American adults reported taking prescription medication for a mental health condition. By 2023, 11.4% of all adults were taking medication specifically for depression. Antidepressants are now the third most commonly prescribed class of drugs in the country. According to CDC data, there are 27 benzodiazepine prescriptions issued for every 100 adults annually, amounting to approximately 66 million physician office visits each year at which a benzodiazepine is prescribed. Prescribing rates for this class of drug nearly doubled between 2003 and 2015. This is not a sustainable solution for the individual, the healthcare system, or the U.S. economy.
And most of this prescribing is not happening with specialist oversight. Research published in Psychiatric Services found that more than 60% of all psychotropic medications are prescribed by providers other than psychiatrists, primarily general practitioners, nurse practitioners, and physician assistants. A Johns Hopkins study found that nearly four in five antidepressant prescriptions are written by non-psychiatrist providers, and that a substantial and growing proportion are prescribed without any accompanying psychiatric diagnosis.
This is not a criticism of primary care physicians working under genuine workforce pressures. There is a real shortage of psychiatrists in the United States and family medicine practitioners are filling an important gap. But it is worth being clear about what this means in practice: most psychiatric medications in this country are being prescribed by clinicians with limited specialist training in brain health, often in brief appointments, working from symptom descriptions, without access to any biological data about the organ they are treating. And rarely equipping people with the tools to understand and actively improve the health of their own brains.
The economic weight of this is equally striking. A 2024 analysis by Deloitte and the Meharry School of Global Health found that unaddressed mental health inequities are already costing the United States more than $477 billion annually in avoidable expenses, factoring in healthcare spillover into conditions like diabetes and cardiovascular disease, lost productivity, unemployment, and widening social inequities. If the current trajectory continues unchanged, cumulative costs are projected to reach $14 trillion by 2040. That equates to roughly $42,000 for every person living in the United States today. This is not a peripheral issue. It sits at the centre of some of the most significant health and economic challenges the country faces.
The Model Was Never Built on Biology
This conversation is not new, and it has not come only from outside the field. In 2009, Thomas Insel, then Director of the National Institute of Mental Health, wrote that the field faced an uncomfortable reality: that current medications help too few people to get better, and very few people to get well.
The research record supports that assessment. A comprehensive review published in Evidence Based Mental Health found that the benefit of antidepressants over placebo is limited, and clinically meaningful primarily in cases of severe depression. For the majority of people prescribed them, those with mild to moderate symptoms, which describes most people who receive them, the pharmacological effect above placebo is marginal.
And perhaps most striking: the core pharmacological agents in use today operate on mechanisms first identified in the 1950s. Chlorpromazine, the first antipsychotic, was introduced in 1952. Decades of research and billions in pharmaceutical investment have not produced agents meaningfully more effective than those early compounds.
The reason is not hard to find. Our psychiatric diagnostic categories were built before functional brain imaging existed. A description of behaviour was never the same thing as an understanding of the underlying biology. For people who respond well to first line treatments, the system works. But for those who cycle through medications, who are told their condition is treatment resistant, who spend years in trial and error, the missing variable is often not a better combination of interventions. It is the biological information that would have pointed toward the right approach from the beginning.
The Brain Deserves the Same Standard
There is a tendency, in medicine and in culture, to treat the brain as somehow separate from the body's biological systems. We talk about mental health in psychological and emotional language, rarely in the same vocabulary of physiology, function, and measurable data that we apply to every other organ.
SPECT imaging challenges that. When you can see seven visually distinct presentations of the same condition laid out in front of you, the abstraction falls away. The brain becomes concrete. The differences are real, specific, and located. And the idea of making significant decisions about someone's neurological health without ever examining their neurology starts to look like what it is: a gap in the standard of care that no other specialty would accept.
The brain governs everything. It deserves at least the same level of investigation we give the heart.
Why Now
Brain health is entering the mainstream in a way it never has before. The science of neuroplasticity, the cognitive effects of chronic stress, the connection between inflammation and mood, the neurological impact of poor sleep: these are no longer niche ideas. The evidence is robust, the conversation is growing, and people are paying attention.
High performing professionals who would never accept a cardiovascular treatment plan based entirely on how they described their symptoms are beginning to ask the same questions about their brains. They want to understand what is actually happening, not just receive a label and a prescription.
That shift is long overdue.
You only know by looking. That principle has always been true in medicine. It is just as true for the brain.
Brain health is not a niche interest. It is the foundation of everything. At Birch Cove, we work with people who are ready to take that seriously. If you are wondering where to begin, a consultation is a good place to start. And if a SPECT scan is something you want to explore, we can walk you through the process and provide access to a preferred referral rate at Amen Clinics. Book a free consultation.
Article References
Suicide statistics
WHO. Suicide Prevention: One person dies every 40 seconds. 2019. https://www.who.int/news/item/09-09-2019-suicide-one-person-dies-every-40-seconds
Hedegaard H, Curtin SC, Warner M. Increase in Suicide Mortality in the United States, 1999–2018. NCHS Data Brief No. 362. CDC/National Center for Health Statistics, 2020. https://www.cdc.gov/nchs/data/databriefs/db362-h.pdf
CDC/NCHS. Suicide Mortality in the United States, 2002–2022. NCHS Data Brief No. 509, 2024. https://www.cdc.gov/nchs/products/databriefs/db509.htm
CDC/NIMH. Suicide Statistics. National Institute of Mental Health, 2023. https://www.nimh.nih.gov/health/statistics/suicide
Cancer mortality decline
USAFacts. US cancer rates and trends: how have cancer rates and mortality changed over time? Citing CDC/NCI data, 2024. https://usafacts.org/articles/how-have-cancer-rates-changed-over-time/
Psychiatric medication prescribing rates
KFF. Exploring the Rise in Mental Health Care Use by Demographics and Insurance Status. 2023. https://www.kff.org/mental-health/exploring-the-rise-in-mental-health-care-use-by-demographics-and-insurance-status/
CDC/NCHS. Prescription Medication for Depression Among Adults: United States, 2023. NCHS Data Brief No. 528, April 2025. https://www.cdc.gov/nchs/products/databriefs/db528.htm
Benzodiazepine prescribing
CDC/NCHS. Physician Office Visits at Which Benzodiazepines Were Prescribed: Findings from 2014–2016 National Ambulatory Medical Care Survey. NCHS Data Brief, 2020. https://pubmed.ncbi.nlm.nih.gov/32510318/
AHRQ. Safe Use of Prescription Benzodiazepines. Effective Health Care Program, 2022. https://effectivehealthcare.ahrq.gov/get-involved/nominated-topics/safe-use-prescription
Non-psychiatrist prescribing
Hughes PM et al. Psychotropic Medication Prescribing Across Medical Providers, 2016–2019. Psychiatric Services. 2024;75(5):477–480. https://psychiatryonline.org/doi/10.1176/appi.ps.20230156
Health Care Cost Institute. Primary Care Providers Prescribe the Majority of Antidepressants and Anxiolytics for People with Employer Sponsored Insurance. HCCI Report, 2023. https://healthcostinstitute.org/all-hcci-reports/primary-care-providers-prescribe-the-majority-of-antidepressants-and-anxiolytics-for-people-with-employer-sponsored-insurance/
Mojtabai R et al. Proportion of Antidepressants Prescribed Without a Psychiatric Diagnosis Is Growing. Health Affairs. 2011;30(8). https://www.healthaffairs.org/doi/10.1377/hlthaff.2010.1024
Johns Hopkins Bloomberg School of Public Health. Prescriptions for Antidepressants Increasing Among Individuals With No Psychiatric Diagnosis. 2011. https://publichealth.jhu.edu/2011/mojtabai-antidepressant-prescriptions
Psychiatric treatment outcomes and efficacy
Insel T. Disruptive Insights in Psychiatry: Transforming a Clinical Discipline. Journal of Clinical Investigation. 2009;119(4):700–705. https://www.jci.org/articles/view/38832
Kirsch I et al. Review: Benefits of Antidepressants Over Placebo Are Limited Except in Very Severe Depression. Evidence-Based Mental Health. 2010;13(2):49. https://ebmh.bmj.com/content/13/2/49
Leucht S et al. Antipsychotic Drugs Versus Placebo for Relapse Prevention in Schizophrenia: A Systematic Review and Meta-Analysis. Lancet. 2012;379(9831):2063–2071. https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(12)60239-6/abstract
Economic burden of mental health
Deloitte Health Equity Institute and Meharry School of Global Health. The Economic Burden of Mental Health Inequities in the United States. 2024. https://www.deloitte.com/us/en/insights/industry/health-care/economic-burden-mental-health-inequities.html
Disclaimer: The information and services provided by Birch Cove are for educational purposes only and are not a substitute for professional medical advice, diagnosis, or treatment. Birch Cove is not a medical provider and does not treat, cure, or prescribe for any medical conditions unless otherwise stated. Always consult your physician or qualified healthcare provider with any medical concerns. Birch Cove assumes no liability for actions taken based on the provided information or services. Product links may be affiliate links, meaning Birch Cove could receive a small commission on purchases.